


Every Sacramento pet owner who has ever come home to a destroyed couch cushion, watched their dog tremble through a thunderstorm, or pulled their hand back from a growl over the food bowl has eventually asked some version of the same question — is this just a training issue, or is something deeper going on? The honest answer, in many cases, is that you may need a vet behaviorist rather than a trainer, and knowing the difference can save you years of frustration and your pet years of suffering. At Del Paso Veterinary Clinic, we have spent decades helping Sacramento families work through anxiety, aggression, compulsive behaviors, and the cognitive changes that come with age, and the single biggest mistake we see is owners trying to “out-train” what is actually a medical problem.
This guide explains the difference between a trainer, a behavioral veterinarian, and a board-certified veterinary behaviorist, when behavioral medication is genuinely appropriate (and when it is not), the most common cases we see in our exam rooms, what an actual behavioral consultation looks like, and how to know when home strategies have stopped working. We have included a real Sacramento case study, a clear comparison table of professional roles, and direct answers to the questions owners ask most.
Reality check from clinical research: A widely cited study published in the Journal of the American Veterinary Medical Association found that behavior-related issues are among the leading reasons dogs are surrendered to shelters in the United States. The vast majority of those surrenders involve behaviors that respond to proper diagnosis and treatment — owners simply did not know help existed.
What Is a Vet Behaviorist, and Why Does the Distinction Matter
The pet professional landscape is genuinely confusing, and most owners do not realize there are at least three different roles people loosely call “behaviorists.” Picking the wrong one wastes months of progress.
The Three Levels of Behavioral Help
Dog Trainers are the entry point. A good trainer teaches obedience, leash manners, recall, and basic problem-solving for normal behavioral wiring — pulling on the leash, jumping on guests, not coming when called. Trainers are not licensed medical professionals. They cannot diagnose anxiety disorders, aggression rooted in pain, or compulsive disorders, and they cannot prescribe anything.
Behavioral Veterinarians (often called “behavioral vets” by Sacramento pet owners searching online) are licensed DVMs who have built a meaningful clinical focus on behavioral medicine within their general practice. They can run bloodwork to rule out thyroid, pain, or neurological causes, prescribe behavioral medications, and create integrated treatment plans that combine medical and behavioral approaches. This is the level of care most pets actually need, and it is what we provide at our clinic.
Board-Certified Veterinary Behaviorists (DACVB) are the top tier — veterinarians who have completed a residency in behavioral medicine and passed board certification through the American College of Veterinary Behaviorists. There are fewer than 100 of them in the entire country. They handle the most complex aggression, severe psychiatric cases, and treatment-resistant patients. Most pets do not need this level. The ones who do are referred by their primary vet.
Why Owners Get Stuck on the Wrong Path
The classic Sacramento pattern looks like this: a dog develops separation anxiety after a household change, the family hires a trainer who teaches “place” command and crate work, the dog still panics when left alone, and the family concludes they have a “bad dog” — when what they actually have is a dog whose nervous system needs medical help alongside behavior modification. By the time they come to us six or twelve months later, the anxiety is more entrenched and harder to unwind. Earlier intervention almost always works better.
Common Behavioral Cases We See in Sacramento
Here are the situations that most often bring families through our doors, in roughly the order of frequency.
Separation Anxiety
Far more common since the pandemic-era schedule changes, separation anxiety in dogs presents as destruction (often near doors and windows), excessive vocalization, pacing, drooling, and sometimes self-harm. The defining feature is that it only happens when the owner is gone — these dogs are usually fine in every other context. Mild cases respond to environmental management and training. Moderate to severe cases need a combination of behavior modification and short-term or long-term medication.
Noise Phobia (Storms, Fireworks, Loud Trucks)
Sacramento’s Fourth of July week and New Year’s Eve are the peak panic seasons for our patients. Dogs with noise phobia tremble, hide, refuse to eat, and sometimes injure themselves trying to escape the sound. According to clinical guidelines from the American Veterinary Medical Association on noise aversions, untreated noise phobias tend to worsen with each exposure, generalizing to wider sound categories over time. Early treatment with situational anti-anxiety medication plus desensitization works dramatically better than waiting.
Aggression
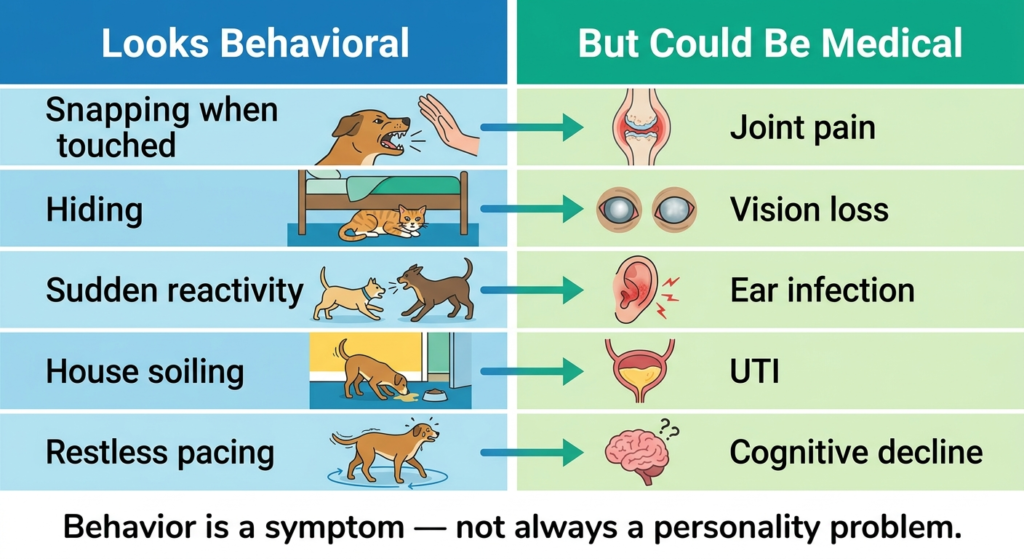
The most consequential category, because the stakes include real bites, lawsuits, and rehoming decisions. Aggression has many root causes — fear, pain, resource guarding, territorial drive, redirected frustration, or, occasionally, a genuine neurological issue. The first job of a behavioral medicine evaluation is figuring out which kind, because each subtype has a different treatment path. Pain-related aggression in particular is widely missed — a dog who suddenly snaps at family members may have arthritis, dental disease, or an ear infection, and no amount of training will fix what is fundamentally a pain problem.
Compulsive Disorders
Tail chasing that goes on for hours, paw licking that creates raw lesions, fly snapping at invisible targets, light or shadow chasing — these repetitive behaviors that the dog cannot self-interrupt are often misdiagnosed as boredom. They are not. True compulsive disorders are neurological, look a lot like human OCD, and respond well to specific medications combined with environmental change.
Cognitive Dysfunction in Senior Pets
The veterinary equivalent of dementia. Senior dogs and cats with cognitive dysfunction get lost in their own homes, reverse their sleep-wake cycle, lose house training, and become anxious or clingy in ways that are not part of who they used to be. A proactive senior pet care plan catches early cognitive changes when they still respond well to treatment, which can include cognitive support medication, dietary changes, and environmental adjustments.
Inter-Pet Aggression in Multi-Pet Households
Two dogs (or two cats) who used to coexist start fighting. The trigger is usually a change — a new pet, an illness in one of them, a household move, even a new piece of furniture. Untreated, these conflicts escalate into serious injuries.
A Real Sacramento Case: Maple’s Storm Anxiety
Maple is a five-year-old border collie mix from East Sacramento whose owner brought her in because she was destroying baseboards during summer thunderstorms — sometimes injuring her paws and gums in the process. The family had hired two trainers and tried multiple over-the-counter calming products. Nothing held up against an actual storm.
Our intake exam ruled out thyroid issues and pain. We diagnosed her with severe noise phobia complicated by anticipatory anxiety, meaning she was already panicking when the barometric pressure shifted, hours before any sound. Her treatment plan combined three layers: a daily background medication to lower her overall anxiety baseline, a fast-acting situational medication to give her family before storm fronts arrived, and a desensitization protocol using recorded thunder at low volumes paired with high-value treats.
By the second summer, Maple was riding out storms in her safe spot under the dining room table without medication on most days, and only needed the situational medication for the worst events. Her family told us the most surprising part of the process was how much calmer she became between storms — which made sense once we understood her nervous system had been running on high alert for years.
When Behavior Problems Are Actually Medical Problems
This is the single most important section of this guide, because it is where most pet owners get derailed.
A meaningful percentage of behavioral cases we evaluate have a medical contributor. Common ones include:
- Pain — arthritis, dental disease, chronic ear infections, intervertebral disc issues
- Thyroid imbalance — hypothyroidism in dogs can cause anxiety, aggression, and personality changes
- Cognitive dysfunction — in senior pets, mimics anxiety and house-soiling issues
- Neurological conditions — seizure disorders, brain tumors (rare but real)
- Sensory decline — vision or hearing loss creates anxiety and startle aggression
- GI discomfort — chronic stomach pain shows up as irritability and food guarding
This is exactly why a proper behavioral workup starts with a physical exam and bloodwork through our in-house diagnostics and lab before any behavioral intervention is prescribed. Skipping this step is how owners end up medicating an anxious dog whose underlying problem is actually back pain.
Comparison: Trainer vs. Behavioral Vet vs. Veterinary Behaviorist
| Role | Credentials | Can Diagnose | Can Prescribe | Best For |
|---|---|---|---|---|
| Dog Trainer | Varies; CCPDT or KPA preferred but unregulated | No | No | Obedience, manners, basic problem behaviors, leash skills |
| Behavioral Vet (DVM with focus) | Licensed veterinarian | Yes | Yes | Anxiety, mild-moderate aggression, compulsions, cognitive issues |
| Board-Certified Veterinary Behaviorist (DACVB) | DVM + 3-year residency + board exam | Yes | Yes | Complex aggression, treatment-resistant cases, severe psychiatric disorders |
| Animal Behaviorist (CAAB / ACAAB) | Graduate degree in animal behavior; not a vet | Limited | No | Behavior modification protocols when paired with veterinary care |
Most pets do best with a combination — a behavioral vet for diagnosis and medication if needed, plus a positive-reinforcement trainer to execute the daily behavior modification work. The two roles complement each other, and good practitioners refer back and forth all the time.
When Behavioral Medication Is Genuinely Appropriate
There is a strong cultural reluctance among Sacramento pet owners to medicate animals. Many of the families we see have already tried calming chews, pheromone diffusers, supplements, weighted vests, and CBD products — sometimes for years — before considering prescription medication.
Modern behavioral medications are not sedatives that flatten your pet’s personality. The good ones (SSRIs, SNRIs, TCAs, situational benzodiazepines, gabapentin for noise events, and a handful of others) work by adjusting the underlying neurochemistry that has gotten stuck in a fear or anxiety loop. When prescribed correctly:
- They give the brain enough relief that behavior modification can actually take hold
- They do not “change who your pet is” — the dog who emerges is the dog who was always there beneath the panic
- They are typically used for 6 to 18 months, then gradually tapered when the dog has built new patterns
- A subset of pets (often those with deeply genetic anxiety) stay on them lifelong, and that is fine
Refusing medication on principle, when a pet is genuinely suffering and behavior modification alone is not working, is the equivalent of refusing pain medication after surgery. The medication is not the goal — quality of life is.
What an Actual Behavioral Consultation Looks Like
Owners often imagine behavior appointments as quick exam-room conversations. They are not. A real consultation typically runs 60 to 90 minutes and covers:
- Detailed history of the behavior — when it started, what triggers it, how often, what has been tried
- Family and household structure — who lives there, who handles the pet, schedule, other pets
- Medical history and current medications
- Physical exam to screen for pain or sensory changes
- Bloodwork when medical contributors are suspected
- Diagnosis and explanation of what is actually happening
- A written treatment plan covering environmental management, behavior modification, training referrals if needed, and medication if appropriate
- Follow-up schedule, usually at two weeks, six weeks, and three months
You will not leave with a quick fix. You will leave with a roadmap.
When to Seek Help vs. When to Wait
Schedule a behavioral consultation when any of the following are true:
- Aggression of any kind, especially toward family members or other pets
- Self-injurious behavior (lick granulomas, broken teeth from cage-bar chewing, paw injuries from escape attempts)
- Anxiety symptoms that persist longer than two weeks despite environmental changes
- Sudden personality changes in adult or senior pets — these almost always have a medical component
- House soiling that is new and unexplained
- Compulsive behaviors that interrupt eating, sleeping, or normal interaction
- Quality of life that is visibly declining
You can reach our team at (916) 925-2107 or visit us at 924 Del Paso Blvd, Sacramento, CA 95815. Same-day appointments are typically available for urgent behavioral concerns, including aggression cases that feel like they may be escalating.
For owners just starting their pet’s journey, our pet wellness exam guide covers the proactive evaluations that often catch early behavioral and medical changes before they become entrenched.
Frequently Asked Questions About Vet Behaviorists and Pet Behavioral Medicine
-
What does a vet behaviorist do that a trainer cannot?
A vet behaviorist can diagnose underlying medical conditions contributing to behavior problems, run bloodwork to rule out thyroid imbalances or pain, prescribe behavioral medications when appropriate, and create integrated treatment plans that address both medical and behavioral components. Trainers focus on teaching skills and modifying observable behavior — they cannot legally diagnose disorders or prescribe medication. For straightforward obedience, a trainer is the right call. For anxiety, aggression, compulsions, or sudden personality changes, a vet behaviorist is the appropriate starting point.
-
How do I find a behavioral vet near me in Sacramento?
Sacramento has several options including general veterinary practices that offer behavioral consultations and a smaller number of board-certified veterinary behaviorists who take referral cases. For most pets, a general practice with a strong behavioral medicine focus and on-site diagnostics is the right level of care. Look for clinics that allocate at least 60 minutes for behavioral consultations, run pre-treatment bloodwork, and combine medication strategies with behavior modification protocols rather than relying on either approach alone.
-
When should I take my dog to a behavioral veterinarian instead of a trainer?
Choose a behavioral veterinarian rather than a trainer when your dog shows aggression of any kind, persistent anxiety despite training efforts, compulsive behaviors, sudden personality changes, self-injurious behavior, or symptoms that started alongside a health change. Choose a trainer when your dog needs basic obedience, leash manners, recall, or help with normal puppy issues like jumping or chewing. Many cases benefit from both — the vet handles the medical and diagnostic side while the trainer executes the day-to-day behavior modification.
-
Are behavioral medications safe for dogs and cats?
Yes, when properly prescribed and monitored. Modern behavioral medications have decades of veterinary use behind them and are well-studied in dogs and cats. Most pets tolerate them very well. Pre-treatment bloodwork screens for liver and kidney function, recheck appointments monitor response and side effects, and dose adjustments fine-tune the result. Side effects, when they occur, are typically mild and resolve with adjustment. The bigger risk is usually the untreated anxiety itself, which causes ongoing physical and emotional harm.
-
How long does behavioral treatment usually take to work?
Timelines depend on the diagnosis. Situational medications for storms or fireworks work within hours of the dose. Daily medications like SSRIs typically take four to six weeks to reach full effect. Behavior modification progress is measured in weeks to months, not days. Most chronic anxiety cases show meaningful improvement at the six to eight week mark, with continued progress over six to twelve months. Compulsive disorders often need longer treatment courses. Your vet should give you realistic milestones at each recheck.
-
Can older pets benefit from behavioral medicine?
Absolutely. Senior pets with cognitive dysfunction, late-onset anxiety, or sudden behavioral changes often respond well to treatment. Cognitive dysfunction in particular is widely undertreated because owners assume the changes are just aging. Specific medications, dietary support, and environmental adjustments can meaningfully improve quality of life for senior dogs and cats showing confusion, sleep cycle changes, or new house-soiling. Earlier intervention generally yields better outcomes, but it is rarely too late to help.
-
What is the difference between a behavioral veterinarian and a board-certified veterinary behaviorist?
A behavioral veterinarian is a licensed DVM who has built clinical expertise in behavioral medicine within their general practice. They handle the majority of cases — anxiety, mild to moderate aggression, compulsions, and cognitive issues. A board-certified veterinary behaviorist (DACVB) has completed an additional three-year residency and passed specialty board examinations. There are very few in the country, and they typically take referral cases involving complex aggression, treatment-resistant disorders, or severe psychiatric presentations. Most pets do well with the first level.
-
How much does a behavioral consultation typically cover?
A proper behavioral consultation is a 60 to 90 minute appointment covering full history intake, physical examination, screening bloodwork when indicated, diagnosis, and a written treatment plan. The treatment plan typically includes environmental management strategies, behavior modification protocols, training referrals when appropriate, and medication if indicated. Follow-up appointments at two weeks, six weeks, and three months track progress and allow medication adjustments. Costs vary based on testing needs and case complexity — your clinic should explain fees during scheduling.
Behavior problems are not character flaws — they are signals from a nervous system asking for help, and the right kind of help can change everything for your pet and for the family who loves them.